
Estimated Read Time: 18 minutes | Target Exam: USMLE Step 1 & Step 2 CK
Why Pharmacology Makes or Breaks Your USMLE Score
Ask any attending who crushed their boards what subject they’d tell their younger selves to master early, and the answer is almost always the same: pharmacology.
Here’s the cold truth: USMLE Step 1 and Step 2 CK both weight pharmacology heavily — roughly 15–20% of total questions on Step 1 alone. That’s not a topic you can skim over. But here’s the flip side — students who truly understand drug mechanisms (not just memorize names) report that pharmacology questions become some of the most predictable and scoreable questions on the entire exam.
This guide gives you what most prep resources don’t: real USMLE-style pharmacology questions with detailed, reasoning-based explanations — the kind that teach you how to think, not just what to memorize.
usmle pathology practice questions step 1
How USMLE Pharmacology Questions Are Actually Structured
Before diving into practice questions, you need to understand how the NBME writes pharm questions. They almost never ask:
“What drug is a beta blocker?”
Instead, they give you a clinical vignette — a patient with symptoms, vitals, lab values — and ask you to:
- Identify the mechanism of action of a drug
- Predict side effects based on mechanism
- Choose the drug with the best risk-benefit profile for a specific patient
- Explain why one drug is contraindicated
The key insight: Every USMLE pharmacology question is really a physiology + pathology + pharmacology hybrid. If you understand why a drug works, you can answer any question they throw at you.
USMLE Pharmacology Questions: High-Yield Categories to Focus On
Based on analysis of NBME free 120, UWorld question banks, and released Step 1/2 content outlines, the following pharmacology categories appear most frequently:
- Autonomic pharmacology (cholinergics, anticholinergics, adrenergics, beta blockers)
- Cardiovascular drugs (antihypertensives, antiarrhythmics, heart failure drugs)
- Antibiotics and antimicrobials (mechanism, resistance, coverage)
- CNS pharmacology (antidepressants, antipsychotics, anesthetics, antiepileptics)
- Renal pharmacology (diuretics)
- Endocrine pharmacology (diabetes drugs, thyroid, steroids)
- Oncology basics (chemotherapy mechanisms)
- Toxicology and antidotes
Let’s work through real practice questions across these categories.
usmle biostatistics practice questions step 1
Practice Question Set: USMLE-Style Pharmacology Questions with Detailed Explanations
🔵 QUESTION 1 — Autonomic Pharmacology (Step 1 Level)
A 55-year-old man with a history of benign prostatic hyperplasia (BPH) and hypertension presents to his physician. His blood pressure is 158/94 mmHg. The physician decides to start a medication that will treat both conditions simultaneously. Which of the following is the most likely mechanism of action of the drug prescribed?
A) Inhibition of angiotensin-converting enzyme
B) Blockade of α1-adrenergic receptors
C) Activation of β2-adrenergic receptors
D) Inhibition of phosphodiesterase-5
E) Blockade of calcium channels in vascular smooth muscle
✅ Correct Answer: B — Blockade of α1-adrenergic receptors
Detailed Explanation:
This question is testing your ability to identify a drug that addresses two separate conditions with one mechanism — a classic USMLE setup.
Let’s break it down:
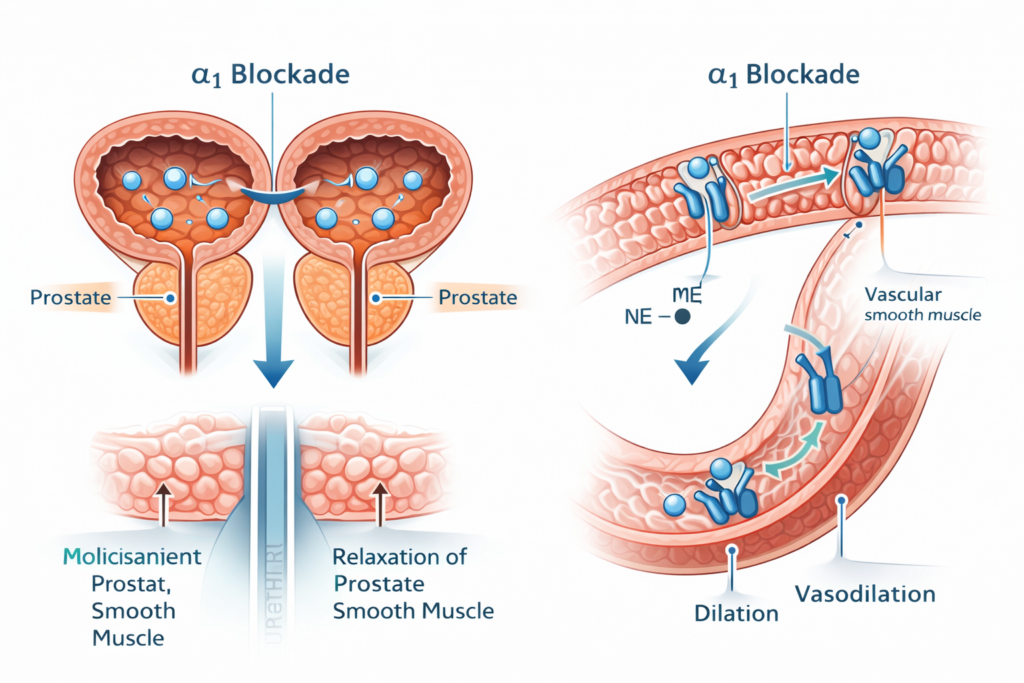
Why α1-blockade works for BPH: The prostate and bladder neck contain α1-adrenergic receptors. When stimulated by norepinephrine, these receptors contract smooth muscle, worsening urinary obstruction. α1-blockers (tamsulosin, terazosin, doxazosin) relax smooth muscle in the prostate and bladder neck → improved urine flow.
Why α1-blockade works for hypertension: α1-receptors are also present in vascular smooth muscle. Blocking them causes vasodilation → decreased peripheral vascular resistance → lower blood pressure.
Drugs in this class: Tamsulosin (more uroselective, better for BPH alone), Terazosin, Doxazosin (less selective, treat both BPH and HTN).
Why the distractors are wrong:
- A (ACE inhibitor): Treats hypertension but has no effect on prostate smooth muscle
- C (β2 agonist): Causes bronchodilation; no role in BPH or hypertension management
- D (PDE-5 inhibitor like sildenafil): Used for erectile dysfunction and pulmonary hypertension; Cialis (tadalafil) has some BPH indication but is not a first-line antihypertensive
- E (Calcium channel blocker): Treats HTN but does not address BPH symptoms
USMLE Test-Taking Tip: Whenever you see BPH + hypertension together in a vignette, immediately think α1-blockers. The NBME loves this combo.
🔵 QUESTION 2 — Cardiac Pharmacology / Antiarrhythmics (Step 1/Step 2 Level)
A 67-year-old woman with a history of atrial fibrillation, COPD, and Type 2 diabetes is being evaluated for rate control therapy. Her resting heart rate is 112 bpm. Which of the following is the most appropriate agent for rate control in this patient?
A) Metoprolol
B) Verapamil
C) Diltiazem
D) Digoxin
E) Amiodarone
✅ Correct Answer: C — Diltiazem
Detailed Explanation:
This is a nuanced clinical pharmacology question requiring you to integrate contraindications with mechanism of action.
The key constraint here is COPD.
Beta-blockers (metoprolol — choice A) are first-line for rate control in atrial fibrillation. However, non-selective beta-blockers and even cardioselective beta-blockers can cause bronchoconstriction in patients with reactive airway disease (COPD, asthma). This makes metoprolol relatively contraindicated in this patient.
Diltiazem is a non-dihydropyridine calcium channel blocker (CCB) that:
- Slows conduction through the AV node → decreases ventricular rate in Afib
- Has no effect on bronchial smooth muscle → safe in COPD
- Also slows SA node firing
Why not verapamil (B)? Verapamil is also a non-DHP CCB with AV nodal blocking effects. It works pharmacologically, but diltiazem is preferred for rate control because verapamil has stronger negative inotropic effects and is more likely to cause heart block. In clinical practice, diltiazem is the go-to non-DHP CCB for Afib rate control.
Why not digoxin (D)? Digoxin slows AV conduction via vagal mechanisms and is useful for rate control, but it’s not first-line for most Afib patients. It’s reserved for patients with heart failure + Afib or those who can’t tolerate other agents. It also has a narrow therapeutic index.
Why not amiodarone (E)? Amiodarone is used for rhythm control (cardioversion and maintaining sinus rhythm), not rate control. It’s also loaded with serious toxicities: pulmonary fibrosis, thyroid dysfunction, hepatotoxicity, corneal microdeposits, photosensitivity. It’s not a first-line rate control agent.
Mnemonics to remember non-DHP CCBs: “Diltiazem and Verapamil = AV nodal blockers” vs. “Dihydropyridines (amlodipine, nifedipine) = peripheral vasodilators only”
usmle mock exam questions free usa
usmle microbiology questions with explanations
usmle step 2 ck practice questions with answers
🔵 QUESTION 3 — Antibiotic Pharmacology (Step 1/Step 2 Level)
A 28-year-old pregnant woman at 16 weeks gestation presents with symptoms of a urinary tract infection. Urine culture grows E. coli sensitive to multiple antibiotics. Which of the following is CONTRAINDICATED in this patient?
A) Nitrofurantoin
B) Cephalexin
C) Amoxicillin
D) Ciprofloxacin
E) Fosfomycin
✅ Correct Answer: D — Ciprofloxacin
Detailed Explanation:
Pregnancy pharmacology is one of the highest-yield topics on USMLE Step 2 CK, and antibiotic safety during pregnancy comes up repeatedly.
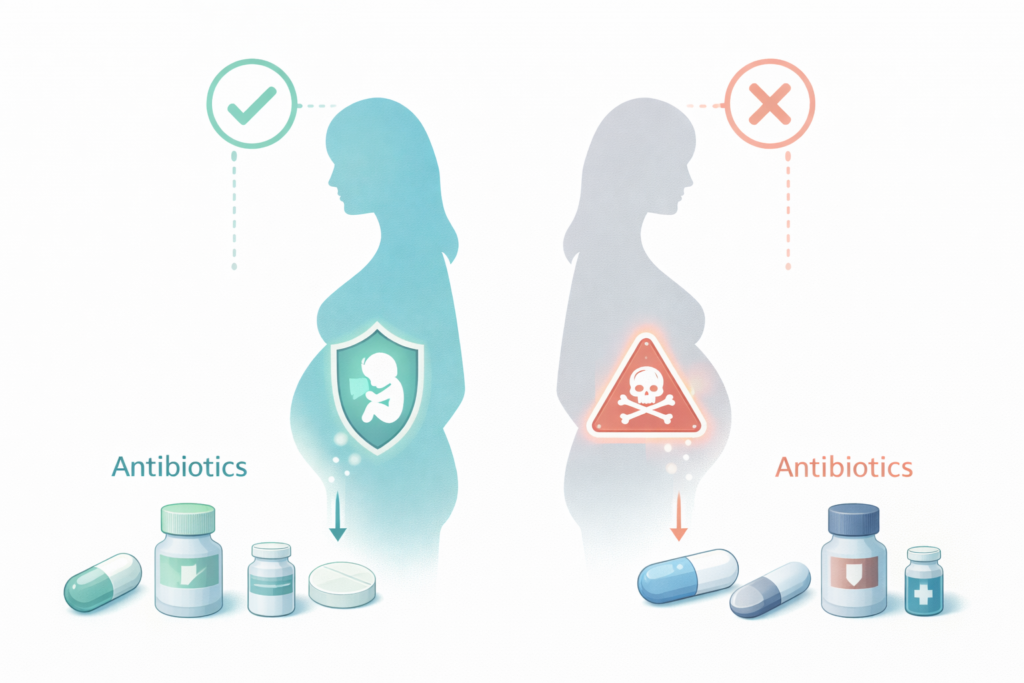
Why ciprofloxacin is contraindicated: Fluoroquinolones (ciprofloxacin, levofloxacin) are FDA Pregnancy Category C/D. The major concern is their documented effect on cartilage and tendon development in animal studies — they deposit in growing cartilage and are associated with arthropathy in developing fetuses. They are avoided throughout pregnancy and in children under 18 (except in specific high-stakes situations like anthrax or serious Pseudomonas infections with no alternatives).
Safe UTI antibiotics in pregnancy (2nd trimester):
- Cephalexin (B): A first-generation cephalosporin. Generally safe throughout pregnancy.
- Amoxicillin (C): A penicillin. Safe in pregnancy (Category B).
- Fosfomycin (E): Single-dose oral antibiotic. Increasingly used for uncomplicated UTIs in pregnancy.
- Nitrofurantoin (A): Safe in 2nd trimester, but avoid in the 1st trimester (teratogenic risk) and at term/near delivery (risk of neonatal hemolytic anemia). At 16 weeks, it’s acceptable.
The classic antibiotic pregnancy contraindications to memorize:
- Fluoroquinolones → Cartilage damage
- Tetracyclines → Teeth discoloration, inhibit bone growth
- Aminoglycosides → Ototoxicity (CN VIII damage)
- Chloramphenicol → “Gray baby syndrome” (near delivery)
- Sulfonamides → Kernicterus (near delivery), neural tube defects (1st trimester)
- Metronidazole → Avoid in 1st trimester
Memory trick: “FLACK” = Fluoroquinolones, Lincosamides (avoid in neonates), Aminoglycosides, Chloramphenicol, Ketolides — generally avoid in pregnancy
🔵 QUESTION 4 — CNS Pharmacology / Antidepressants (Step 2 CK Level)
A 34-year-old man with major depressive disorder is started on a new antidepressant. Two weeks later, he presents to the ER with agitation, diaphoresis, tremor, hyperreflexia, and hyperthermia. He mentions he also took St. John’s Wort for “extra support.” What is the most likely diagnosis, and what drug combination caused it?
A) Neuroleptic malignant syndrome; antipsychotic + anticholinergic
B) Serotonin syndrome; SSRI + St. John’s Wort
C) Anticholinergic toxicity; TCA + antihistamine
D) Tyramine reaction; MAOI + aged cheese
E) Extrapyramidal symptoms; SSRI + dopamine antagonist
✅ Correct Answer: B — Serotonin syndrome; SSRI + St. John’s Wort
Detailed Explanation:
This is a clinical presentation question that tests your ability to:
- Recognize the clinical syndrome
- Identify the causative drug interaction
Serotonin Syndrome Triad:
- Altered mental status (agitation, confusion)
- Autonomic instability (diaphoresis, hyperthermia, tachycardia)
- Neuromuscular abnormalities (hyperreflexia, tremor, clonus, myoclonus)
The critical distinguishing feature between serotonin syndrome and NMS is hyperreflexia and clonus (serotonin syndrome) vs. lead-pipe rigidity (NMS).
The Drug Interaction: SSRIs (sertraline, fluoxetine, escitalopram) block the serotonin reuptake transporter (SERT). St. John’s Wort (Hypericum perforatum) is an herbal supplement that also inhibits SERT as well as having MAOI-like properties. Combining them leads to excessive serotonergic activity.
Other dangerous serotonin syndrome combinations:
- SSRI + MAOI (most dangerous — absolute contraindication)
- SSRI + Tramadol (tramadol inhibits serotonin reuptake)
- SSRI + Linezolid (linezolid has weak MAOI properties)
- SSRI + Triptans (serotonin agonists — controversial but recognized risk)
- SSRI + Dextromethorphan (DXM — found in cough syrups)
Treatment of Serotonin Syndrome:
- Discontinue causative agents
- Benzodiazepines (for agitation and seizures)
- Cyproheptadine (serotonin antagonist — the antidote)
- Supportive care: cooling, IV fluids
Why the other choices are wrong:
- A (NMS): Would present with muscle rigidity, bradyreflexia, gradual onset over days — and involves antipsychotics/dopamine blockade
- C (Anticholinergic toxicity): “Hot as a hare, dry as a bone, red as a beet, blind as a bat, mad as a hatter” — no hyperreflexia, skin is dry not diaphoretic
- D (Tyramine reaction): Occurs with MAOIs + tyramine-rich foods → hypertensive crisis — no muscle findings
- E: SSRIs don’t cause EPS
🔵 QUESTION 5 — Diuretics (Step 1 Level)
A 62-year-old man with heart failure and chronic kidney disease (GFR 22 mL/min/1.73m²) presents with worsening peripheral edema. Which diuretic is most appropriate for this patient?
A) Hydrochlorothiazide
B) Acetazolamide
C) Furosemide
D) Spironolactone
E) Triamterene
✅ Correct Answer: C — Furosemide
Detailed Explanation:
This question requires understanding how kidney function affects diuretic efficacy — a concept that is highly testable.
Why furosemide: Loop diuretics (furosemide, bumetanide, torsemide) work at the thick ascending limb of the Loop of Henle, blocking the Na-K-2Cl cotransporter. They are the most potent diuretics and — crucially — remain effective in patients with reduced GFR, making them the diuretic of choice in CKD and heart failure.
Why NOT thiazides (A): Thiazides (hydrochlorothiazide, chlorthalidone) work at the distal convoluted tubule and require adequate renal function to work. They lose efficacy when GFR drops below ~30 mL/min. At a GFR of 22, thiazides are largely ineffective.
Why NOT acetazolamide (B): This is a carbonic anhydrase inhibitor working at the proximal tubule. It’s used for altitude sickness, glaucoma, and metabolic alkalosis — not for edema in heart failure.
Why NOT spironolactone (D) or triamterene (E): Potassium-sparing diuretics are relatively contraindicated in CKD because CKD impairs potassium excretion. Adding these agents risks dangerous hyperkalemia. Note: Spironolactone has a mortality benefit in heart failure at low doses, but must be used very cautiously with close potassium monitoring when GFR is this low.
Key diuretic pharmacology table:
| Diuretic | Site of Action | Use | Watch For |
|---|---|---|---|
| Furosemide | Loop of Henle | Edema, HTN, HF, CKD | Hypokalemia, ototoxicity |
| HCTZ | Distal tubule | Hypertension, hypercalciuria | Hypokalemia, hyperglycemia |
| Spironolactone | Collecting duct | HF, hyperaldosteronism | Hyperkalemia, gynecomastia |
| Acetazolamide | Proximal tubule | Glaucoma, altitude sickness | Metabolic acidosis |
| Mannitol | Proximal tubule | ICP, acute glaucoma | Volume overload initially |
USMLE Step 1 Glomerulonephritis Pathology Questions
🔵 QUESTION 6 — Toxicology / Antidotes (Step 1 & Step 2 Level)
A 3-year-old is brought to the ER after ingesting an unknown substance from the garage. On exam: pinpoint pupils, excessive salivation, lacrimation, urination, defecation, bradycardia, and bronchospasm. What is the appropriate antidote?
A) N-acetylcysteine
B) Flumazenil
C) Naloxone
D) Atropine
E) Physostigmine
✅ Correct Answer: D — Atropine
Detailed Explanation:
This is a classic organophosphate/cholinergic toxicity presentation, and the USMLE loves toxicology questions because they combine mechanism, clinical recognition, and treatment all in one.
Recognizing the Syndrome — “SLUDGE + DUMBELS”:
The muscarinic (parasympathetic) effects of excess acetylcholine:
- Salivation
- Lacrimation
- Urination
- Defecation
- GI cramps
- Emesis
- Defecation, Urination, Miosis, Bradycardia, Emesis, Lacrimation, Secretions
Pinpoint pupils (miosis) + bradycardia + excessive secretions = cholinergic toxidrome from organophosphate poisoning (common in pesticides/insecticides) or nerve agent exposure.
Mechanism of Organophosphate Toxicity: Organophosphates irreversibly inhibit acetylcholinesterase → buildup of ACh at all synapses → overstimulation of muscarinic AND nicotinic receptors.
Treatment:
- Atropine (muscarinic antagonist) — First and most critical. Blocks muscarinic receptors → reverses bronchospasm, bradycardia, secretions. Give until secretions dry up (endpoint is dry lungs). Doses can be massive (2–4 mg IV, repeated).
- Pralidoxime (2-PAM) — Must be given early, before “aging” (irreversible binding becomes permanent). Pralidoxime regenerates acetylcholinesterase and addresses the nicotinic effects (muscle weakness, paralysis) that atropine doesn’t cover.
Why the distractors are wrong:
- A (N-acetylcysteine): Antidote for acetaminophen overdose — replenishes glutathione
- B (Flumazenil): Reverses benzodiazepine overdose
- C (Naloxone): Reverses opioid overdose — look for respiratory depression, miosis, but no secretions or bradycardia
- E (Physostigmine): This is a cholinesterase inhibitor — it would WORSEN this patient. Physostigmine is used for anticholinergic toxicity (the opposite problem)
USMLE Antidote Quick Reference:
| Toxin | Antidote |
|---|---|
| Acetaminophen | N-acetylcysteine |
| Opioids | Naloxone |
| Benzodiazepines | Flumazenil |
| Organophosphates | Atropine + Pralidoxime |
| Anticholinergics | Physostigmine |
| Heparin | Protamine sulfate |
| Warfarin | Vitamin K, FFP |
| Methanol/Ethylene glycol | Fomepizole (or ethanol) |
| Iron | Deferoxamine |
| Lead | DMSA (succimer) |
| Digoxin | Anti-digoxin Fab antibodies |
| Beta-blocker OD | Glucagon, high-dose insulin |
usmle step 1 practice questions with explanations free
High-Yield USMLE Pharmacology Concepts That Students Miss
1. First-Pass Effect and Bioavailability
The USMLE tests whether you know why certain drugs must be given IV vs. orally. Drugs with high first-pass metabolism (lidocaine, nitroglycerin, morphine, propranolol) have significantly reduced bioavailability when swallowed. This is why:
- Nitroglycerin is given sublingual or transdermal
- Lidocaine cannot be given orally for arrhythmias
2. Zero-Order vs. First-Order Kinetics
First-order kinetics: A constant fraction of drug is eliminated per unit time. Most drugs follow this. Half-life is constant.
Zero-order kinetics: A constant amount is eliminated per unit time regardless of concentration — because elimination enzymes are saturated. Examples: Phenytoin, Ethanol, Aspirin (at high doses). This is dangerous because small dose increases cause disproportionately large increases in plasma levels.
3. Cytochrome P450 Interactions — The Yield Is High
CYP450 interactions are responsible for a significant number of USMLE pharmacology questions.
CYP Inducers (decrease drug levels): “PC BRAS” — Phenytoin, Carbamazepine, Barbiturates, Rifampin, Alcohol (chronic), St. John’s Wort
CYP Inhibitors (increase drug levels → toxicity): “SICKFACES.COM” — Sodium valproate, Isoniazid, Cimetidine, Ketoconazole, Fluconazole, Azithromycin/Amiodarone, Ciprofloxacin, Erythromycin, Sulfonamides, Chloramphenicol, Omeprazole, Metronidazole
4. Receptor Pharmacology Terminology
Questions often present clinical scenarios where you must identify if a drug is an agonist, partial agonist, competitive antagonist, or non-competitive antagonist:
- Full agonist: Activates receptor maximally (morphine)
- Partial agonist: Activates receptor, but less than maximally; also blocks full agonist when both present (buprenorphine)
- Competitive antagonist: Reversible blockade; can be overcome by increasing agonist concentration (naloxone vs. morphine; the dose-response curve shifts right but Emax unchanged)
- Non-competitive antagonist: Irreversible binding; Emax is reduced (phenoxybenzamine)
How to Study USMLE Pharmacology Effectively: A Proven Strategy
Step 1: Learn Mechanisms First, Names Second
Don’t start by memorizing drug names. Start by understanding the receptor, enzyme, or transporter the drug targets. Ask: “What happens physiologically when I activate or block this target?”
Step 2: Use First Aid Strategically
First Aid for the USMLE Step 1 has an excellent pharmacology section. But don’t read it passively. After reading about each drug class, cover the page and try to recall mechanism, indications, side effects, and contraindications.
Step 3: Do UWorld Questions by Organ System
UWorld’s pharmacology questions are among the highest-quality USMLE prep questions available. Don’t do them in “random” mode early in your studying — do them by organ system so you reinforce pathology + pharmacology together.
Step 4: Build Your Own Antidote and Side Effect Lists
Create flashcards (Anki works beautifully here) for:
- Drug-specific toxicities (e.g., bleomycin → pulmonary fibrosis)
- Drug antidotes
- Drugs to avoid in specific populations (pregnancy, renal failure, hepatic failure)
Step 5: Tackle CYP450 and Drug Interactions Last (Not First)
Students often waste time memorizing CYP tables early when they don’t have enough clinical context. Learn the major inducers and inhibitors after you understand the drugs they interact with.
The Most Commonly Tested Drug Side Effects on USMLE
These side effects appear across multiple exam questions and are non-negotiable to memorize:
| Drug | Unique Toxicity |
|---|---|
| Amiodarone | Pulmonary fibrosis, thyroid dysfunction, corneal deposits, photosensitivity, blue-gray skin |
| Clozapine | Agranulocytosis (requires WBC monitoring) |
| Lithium | Nephrogenic diabetes insipidus, thyroid, narrow therapeutic index |
| Metformin | Lactic acidosis (rare, especially with renal failure) |
| ACE inhibitors | Dry cough (bradykinin), angioedema |
| Statins | Myopathy/rhabdomyolysis (especially with CYP3A4 inhibitors) |
| Fluoroquinolones | Tendon rupture, QT prolongation, avoid in children/pregnancy |
| Tetracyclines | Teeth discoloration, photosensitivity, avoid in pregnancy |
| Vancomycin | “Red Man Syndrome” (infusion-related, not allergy), nephrotoxicity, ototoxicity |
| Cisplatin | Nephrotoxicity, peripheral neuropathy, ototoxicity |
| Bleomycin | Pulmonary fibrosis |
| Doxorubicin | Dilated cardiomyopathy (dose-dependent) |
Quick Quiz: Test Yourself
Before moving on, try these rapid-fire questions (answers below):
- Which beta-blocker is used specifically for hypertrophic obstructive cardiomyopathy (HOCM)?
- A patient on isoniazid develops peripheral neuropathy. What is the treatment?
- What is the mechanism of action of metformin?
- Which antiepileptic drug is first-line for absence seizures?
- What reverses heparin overdose?
Answers:
- Propranolol (non-cardioselective; decreases outflow tract obstruction by reducing heart rate and contractility)
- Pyridoxine (Vitamin B6) — INH depletes B6, causing neuropathy
- Activates AMPK → decreases hepatic gluconeogenesis; also improves insulin sensitivity
- Ethosuximide (blocks T-type calcium channels in thalamic neurons)
- Protamine sulfate
Conclusion: Mastering USMLE Pharmacology Questions
The students who score highest on pharmacology sections of the USMLE aren’t those with the best memory — they’re those with the deepest mechanistic understanding. Every drug question on the USMLE can be reasoned through if you understand:
- What receptor/enzyme/transporter does the drug target?
- What is the normal physiological role of that target?
- What happens when you activate or block it?
- What patient characteristics change the risk-benefit calculation?
Practice questions aren’t just assessment tools — they’re learning tools. Read every explanation, even for questions you got right. The USMLE question writers have patterns, and the more you recognize those patterns, the more predictable the exam becomes.
Keep going. The white coat is worth it.
Disclaimer: This article is intended as an educational resource for USMLE exam preparation and does not constitute medical advice. Clinical decision-making should always be guided by licensed healthcare professionals and current clinical guidelines.